The 1832 & 1848-49 Cholera Epidemics
Examining disease transmission, mortality, and the early public health response in Belfast
Arrival and medical understanding of cholera
On 28 February 1832, Bernard Murtagh, a 34-year-old cooper living in a lodging house on Quay Lane, Belfast—a narrow street near the River Lagan—became violently ill. Described as a man of "irregular habits," he had suffered from diarrhoea for two or three days previously but had reported no other symptoms when he went to bed after his usual supper of stirabout and milk. Around midnight his condition deteriorated sharply as he experienced acute vomiting and diarrhoea. The violently expelled fluid was described as whitish, resembling milk, or meal and water. By the morning, Bernard was also suffering from intense cramps. He was seen by Surgeon McBurney and members of the Belfast Board of Health, who found him in a state of extreme collapse: profoundly weak, extremely cold, and without a perceptible pulse at the wrist. A mustard emetic was administered around midday after which he appeared to revive slightly. However, this improvement was only temporary, and he died between 7 and 8 p.m. that evening, some nineteen hours after becoming ill.

Bernard had become the first recognised victim in Ireland to have died from what was then perceived by westerners as a new and alarming global pandemic that had originated from the East: Asiatic cholera. Noted for its severity, rapidity and high mortality, cholera had long been endemic in India before spreading across Asia after 1817 and into Europe after 1829. Its signature symptoms were both distinctive and terrifying: violent vomiting and diarrhoea, resembling rice water or husks, was typically accompanied by agonising cramps, muscular spasms, a weakened pulse, low temperature, and a blue tinge to the nails and skin. Death could follow within hours.
The disease is now understood to be caused by the microorganism, Vibrio Cholerae usually transmitted through the ingestion of water contaminated by the excreta of infected individuals, particularly in urban environments where infected sewage was able to contaminate the public water supply. In the towns and cities of nineteenth century Ireland, where sanitary practices and sewerage infrastructure were often rudimentary, this particular mode of transmission made cholera a particularly deadly hazard.
Cholera Mortality in Ireland
Belfast Mortality Rates
- 1832: 2,831 cases / 418 deaths
Mortality: 14.8% - 1848-49: 3,538 cases / 1,163 deaths
Mortality: 33%
Across Ireland, around forty per cent of those who contracted cholera between 1832 and 1833 died, with mortality rates in some localised outbreaks reaching as high as seventy-six per cent. In the second epidemic, which occurred between 1848 and 1849, mortality rates in many areas were even higher, as the disease spread through a population which had been severely weakened by the Great Famine and its associated illnesses. In 1832, however, Belfast's mortality rate stood at 14.8 per cent, considerably lower than the national average and significantly better than the rates recorded in Dublin and Cork, both of which exceeded forty per cent. Those most vulnerable, however, were more immediately affected by the underlying deficiencies of Belfast's urban environment.
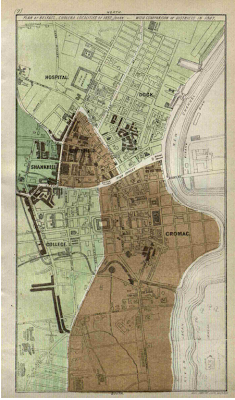
Belfast's Urban Environment
Nineteenth-century Belfast was Ireland's only industrialised town and outwardly appeared prosperous and successful. One contemporary observer described it as if it "had money in its pocket and roast beef for dinner." Yet this image of prosperity masked a town in which industrial expansion had outpaced basic urban infrastructure, particularly in the provision of housing, water supply, and sanitation. Behind its well-appointed main streets lay a dense and poorly regulated network of confined and insanitary backstreets consisting of courts, lanes, and alleys. Housing for the labouring poor was arranged in a grid pattern of tightly confined plots with minimal drainage or ventilation and commonly consisted of two-storey buildings occupied by two or more families. Water supply was similarly limited: few homes were provided with piped water, and over 7,000 houses were supplied from public fountains, water carts, or pumps sunk by landlords. At the same time, sewers were often constructed to discharge their effluent directly into adjacent watercourses. During high tides or periods of flooding, this waste was carried back onto the streets and into nearby homes, worsening already precarious sanitary conditions and increasing the risk of disease.
The 1832 Epidemic in Belfast
When cholera came however, Belfast appeared to have been as well, if not better prepared to combat the disease than most. The initial response was coordinated by the towns Police Commissioners and a somewhat ad hoc and hastily formed Board of Health. Working closely together, they implemented a systematic programme of street cleaning, fumigation and whitewashing houses, while also providing food, clothing and bedding for those most in need. Temporary hospital accommodation was established in the grounds of Belfast's Fever Hospital, with Dr Henry McCormac placed in charge. McCormac combined a strict isolation policy with treatments which included bloodletting and the administration of calomel (mercury), opiates and dilute sulphuric acid. These interventions, grounded in contemporary medical theory, formed the principal therapeutic response available at the time, but they were frequently unsuccessful. Still, while mortality rates within the hospital were higher (22%) than Belfast's overall figures, the town did not experience the same level of resistance to hospital admission than was seen elsewhere. In Dublin, for example, public hostility towards removal to hospital sometimes escalated into violence and carriages carrying the sick were occasionally set upon, the patients 'rescued' and the vehicles subsequently thrown into the River Liffey.
By the end of the first epidemic cholera had caused approximately 2,831 cases and 418 deaths in Belfast and the town's 14.8 per cent mortality rate was considerably better than many other comparably sized towns in Britain and Ireland. Therefore, the management of the epidemic by Belfast's civic and medical authorities can be regarded as a relative success. However, the failure to sustain public health intervention beyond this crisis meant that, when cholera recurred, the town faced a significantly more severe outbreak, one that starkly revealed the limited extent of civic improvement in precisely those areas where it was most urgently needed.
The 1848-49 Cholera Epidemic
By the mid-1840s, cholera and the commitment to sustained proactive public health provision had largely faded from public consciousness in Belfast. With social and medical attention now focused on the devastating effects of the Great Famine and associated diseases such as typhus fever, when cholera returned to Ireland in 1848, there had been little advancement in the approach to the disease. Although a new Poor Law and its accompanying workhouse infrastructure had ushered in a new era of state regulated institutional care and civic response to crises, central response tended to be reactionary. Thus, the success of cholera response required proactive measures to be implemented at a local level. In Belfast, it was the efforts of Belfast's new Board of Guardians, the physician and sanitary reformer Dr Andrew Malcolm and additional sanitary powers granted to the new Town Corporation by town improvement legislation which arguably prevented significantly higher mortality than was experienced elsewhere.
As early as 1841 Belfast's Guardians acted in defiance of the Poor Law Commissioners when they opened the Belfast Workhouse with ten beds set aside for the reception of the sick, rapidly increasing this to 100. Between 1845 and 1847 a series of new Town Improvement Acts permitted the Belfast Corporation to introduce new housing regulations and implement additional sanitary powers which gave them more authority to require landlords and property owners to remove nuisances, pave streets and improve sanitation. By 1848 however, Dr Malcolm reported that there continued to be a 'lamentable deficiency' with regard to the removal of offensive remains and with anxiety growing in regard to a potential cholera epidemic the influential physician rose to the fore to guide the response of the town's civic authorities. A Sanitary Committee headed by Malcolm and specifically aimed at dealing with cholera in the first instance was formed in 1848. The Committee published and distributed reports, saw that magistrate's orders were issued for the removal of nuisances, constructed sewers in some areas and helped to provide poor families with fresh bedding in addition to whitewashing houses.
Yet, despite these preparations, mortality by the end of the 1849 epidemic was almost three times higher than it had been in 1832. Although Belfast had two hospitals capable of receiving cholera patients, the Union Fever Hospital and the General Hospital, the willingness of the sick to seek admission had declined markedly since the previous decade. The committee of the General Hospital attributed this reluctance to widespread prejudices and to the apathy and hopelessness that typically accompanied the disease and expressed regret that the advantages offered by the hospital were not more widely appreciated by the poor.
The 1848–49 epidemic resulted in approximately 3,538 cases and 1,163 deaths in Belfast. This represented a significant increase in both cases and fatalities compared with the 1832 outbreak; however, the mortality rate of thirty-three per cent was again lower than that recorded in many other comparable Irish towns. In Belfast's worst-affected districts, poverty and persistent deficiencies in sanitation and hygiene clearly played a central role in the spread of the disease. While the town's municipal authorities had carried out considerable civic improvements, major sanitary works had still not been implemented in the areas where they were most urgently needed. Some lasting lessons were nevertheless learned. When cholera returned in 1853 and 1866, case numbers fell markedly, yet, because medical understanding remained limited and treatment practices largely unchanged, mortality remained high, demonstrating that sanitary reform alone was insufficient to overcome the constraints of nineteenth-century medicine.
© Dr Nigel Farrell — This work is shared for research and educational purposes. Any reuse, quotation, or reproduction must include appropriate academic attribution to the author. The content may not be redistributed commercially without permission. Full licence details →